
Most coronary heart assaults are attributable to nonobstructive plaques that infiltrate your entire coronary artery tree. There isn’t a such factor as “1-vessel illness,” “2-vessel illness,” or “left predominant illness.” Atherosclerotic plaque is steady all through the coronary arteries of coronary heart assault victims.
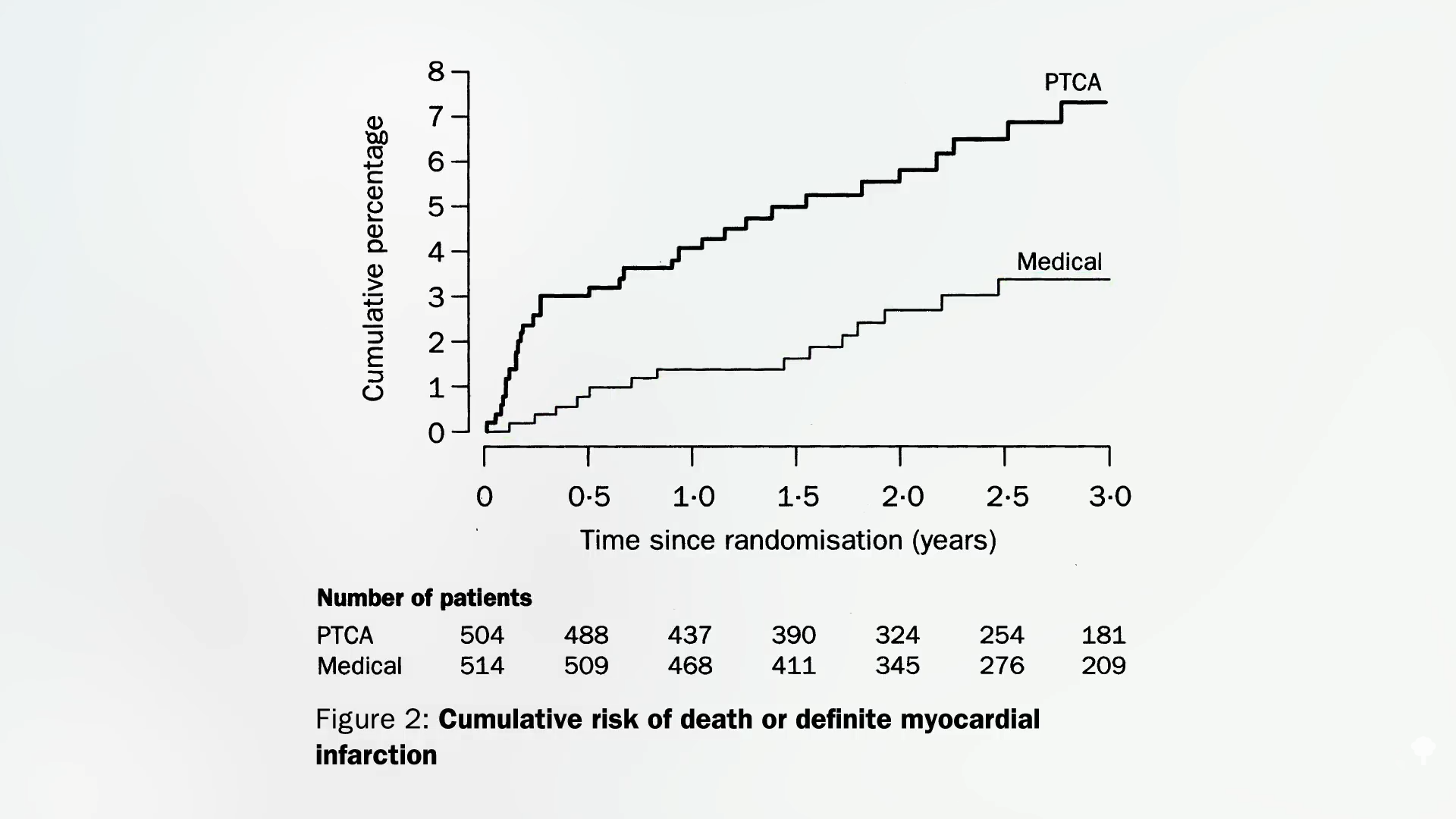
In angioplasty, a tiny balloon is inserted right into a narrowed coronary artery that feeds the guts to pressure it to open wider to enhance blood stream. It wasn’t put to the take a look at in a randomized managed trial till 1992. It not solely failed to forestall coronary heart assaults, nevertheless it additionally failed to point out any survival profit. Nonetheless, the researchers solely adopted sufferers for six months and included folks with comparatively minor illnesses who may not have been sick sufficient to profit from the process. Enter the MASS trial. Researchers enrolled these with extreme blockage excessive up of their left anterior descending coronary artery—the widow-maker or widower-maker (since coronary artery illness can also be the primary killer of girls)—and adopted them for years. The findings? There was no distinction in subsequent mortality or coronary heart assault charges. There have been solely about 200 sufferers in that trial, although. Possibly the profit was so refined {that a} better variety of sufferers had been wanted to tease out the impact. Enter the RITA-2 examine, which randomized greater than a thousand sufferers. Researchers did certainly discover a clear distinction within the danger of future demise and coronary heart assault, nevertheless it was within the flawed path. The angioplasty group suffered twice the danger in comparison with these randomized to forgo surgical procedure, as proven under and at 1:18 in my video Why Angioplasty Coronary heart Stents Don’t Work Higher.
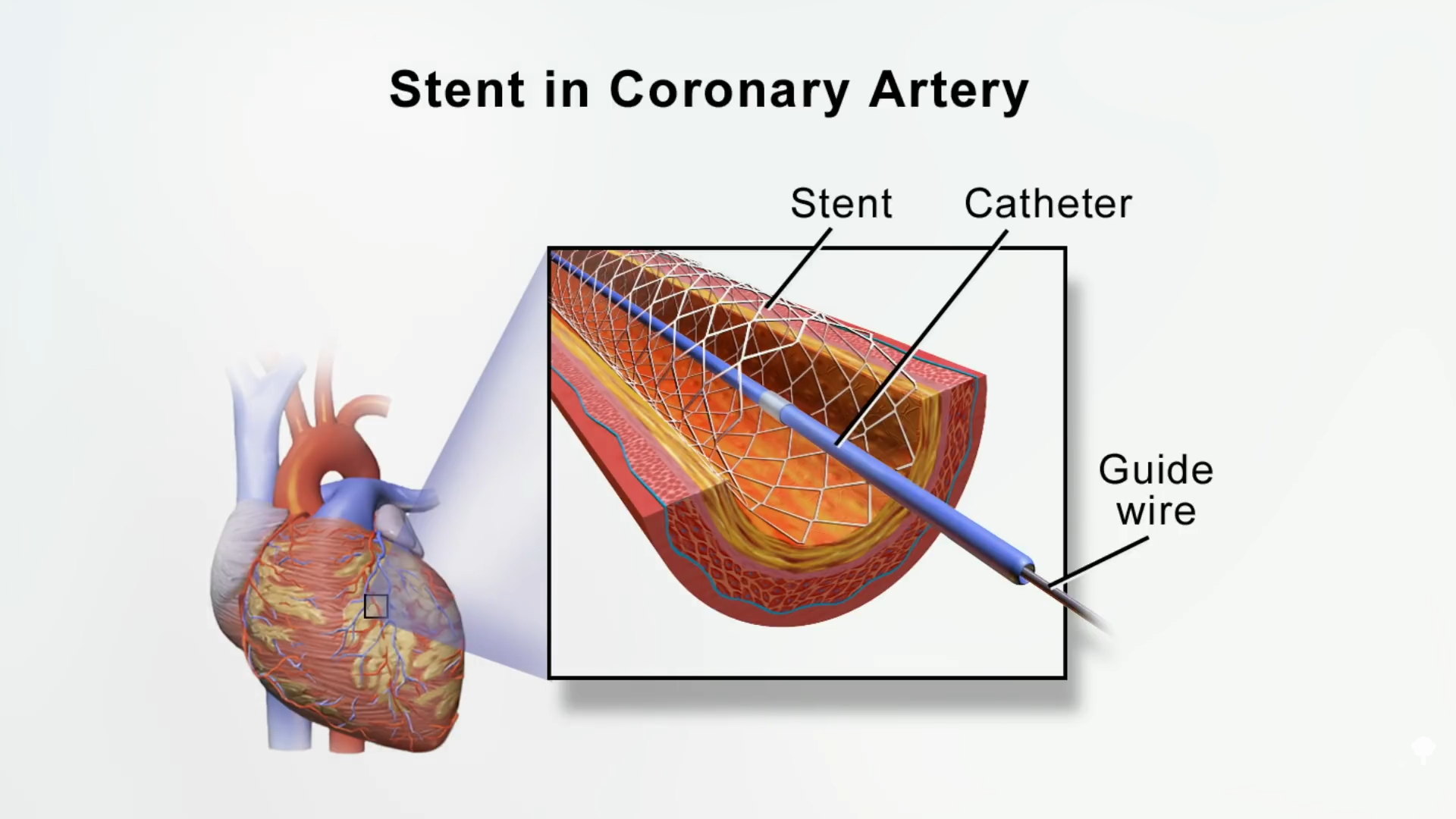
This was all earlier than stents got here into vogue, although. As a substitute of simply ballooning up the artery, how about completely inserting a stent, a metallic mesh tube, to prop open the artery, as you possibly can see right here and at 1:33 in my video? Absolutely, that’s acquired to assist.
Enter the MASS-II trial, which, once more, noticed no profit after one 12 months—however no profit was seen after 5 years and even ten years. Then got here the Braveness Trial, which randomized hundreds of sufferers, and it, too, fell flat on its face.
These largely used naked metallic stents, although, not the newer “drug-eluting” ones that launch medicine slowly. And what about high-risk teams, reminiscent of these recognized with diabetes and different extra severe illnesses, or those that have one hundred pc blocked arteries days after having a coronary heart assault? In meta-analysis after meta-analysis, trying at 5 trials with 5,000 sufferers, there was no discount in demise, coronary heart assault, and even angina ache. In ten trials with greater than 6,000 sufferers, there was no profit for survival, coronary heart assaults, or ache aid. Now, we’re as much as greater than a dozen main trials and nothing: no profit from angioplasty and stents. “Moreover, a number of analyses have did not establish a single high-risk subset that advantages…” How is that attainable? You’re bodily opening up blood stream.
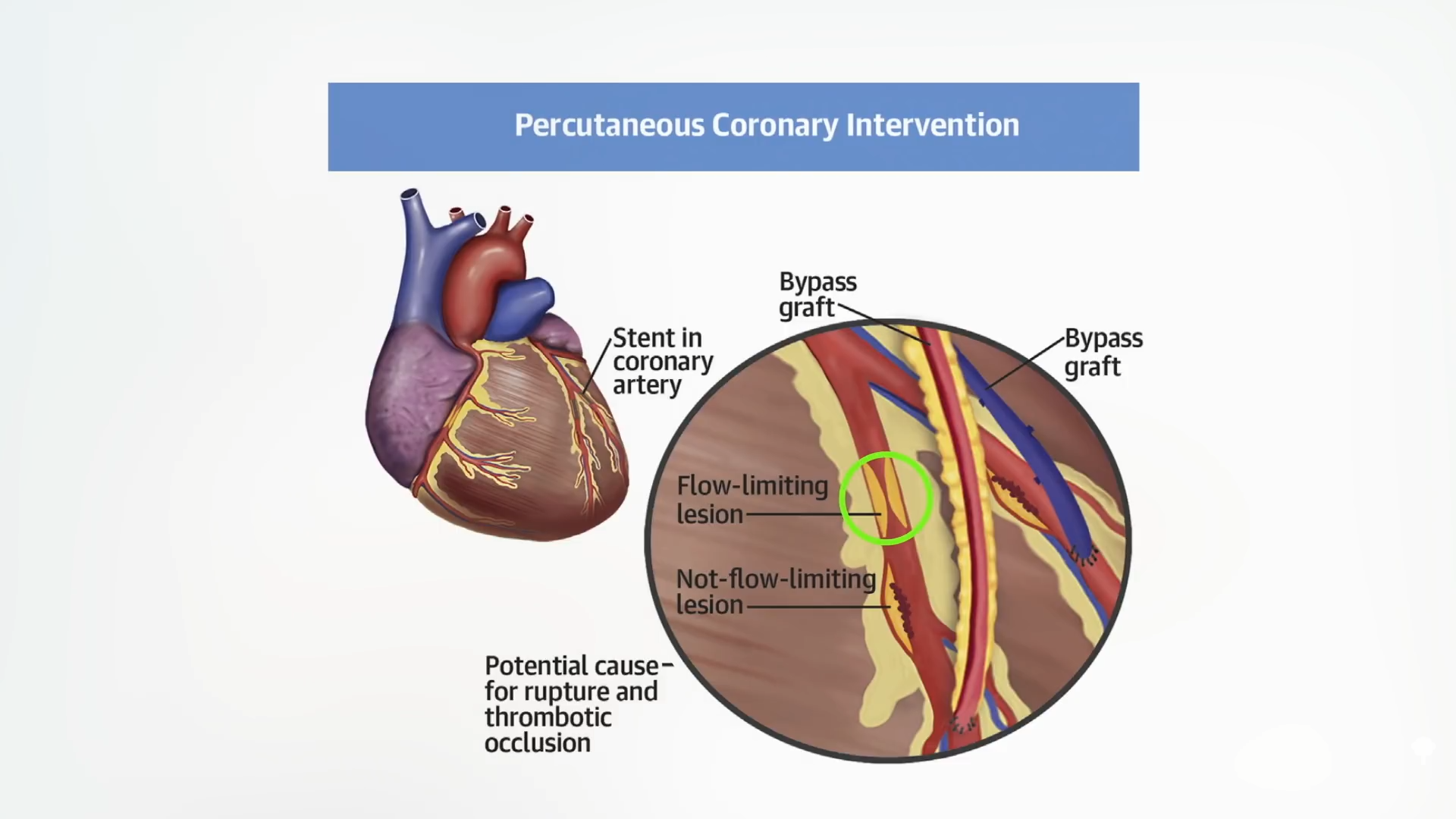
The rationale it doesn’t work is that almost all of coronary heart assaults in actual life are attributable to narrowings lower than 70 p.c—“i.e., probably non-flow-limiting lesions”—so the plaques in our arteries that kill us have a tendency to not be those which are limiting blood stream. Proven under and at 3:21 in my video are two atherosclerotic plaques. The one circled in inexperienced and labeled “Move-limiting lesion” is squeezing off the blood stream a lot that it may be seen on an angiogram and docs can go after it with a stent.
Drawback solved and life saved, proper? No, as a result of it was the invisible one (circled in yellow under) that wasn’t even impeding blood stream that was going to kill us all alongside, as you possibly can see right here and at 3:27.
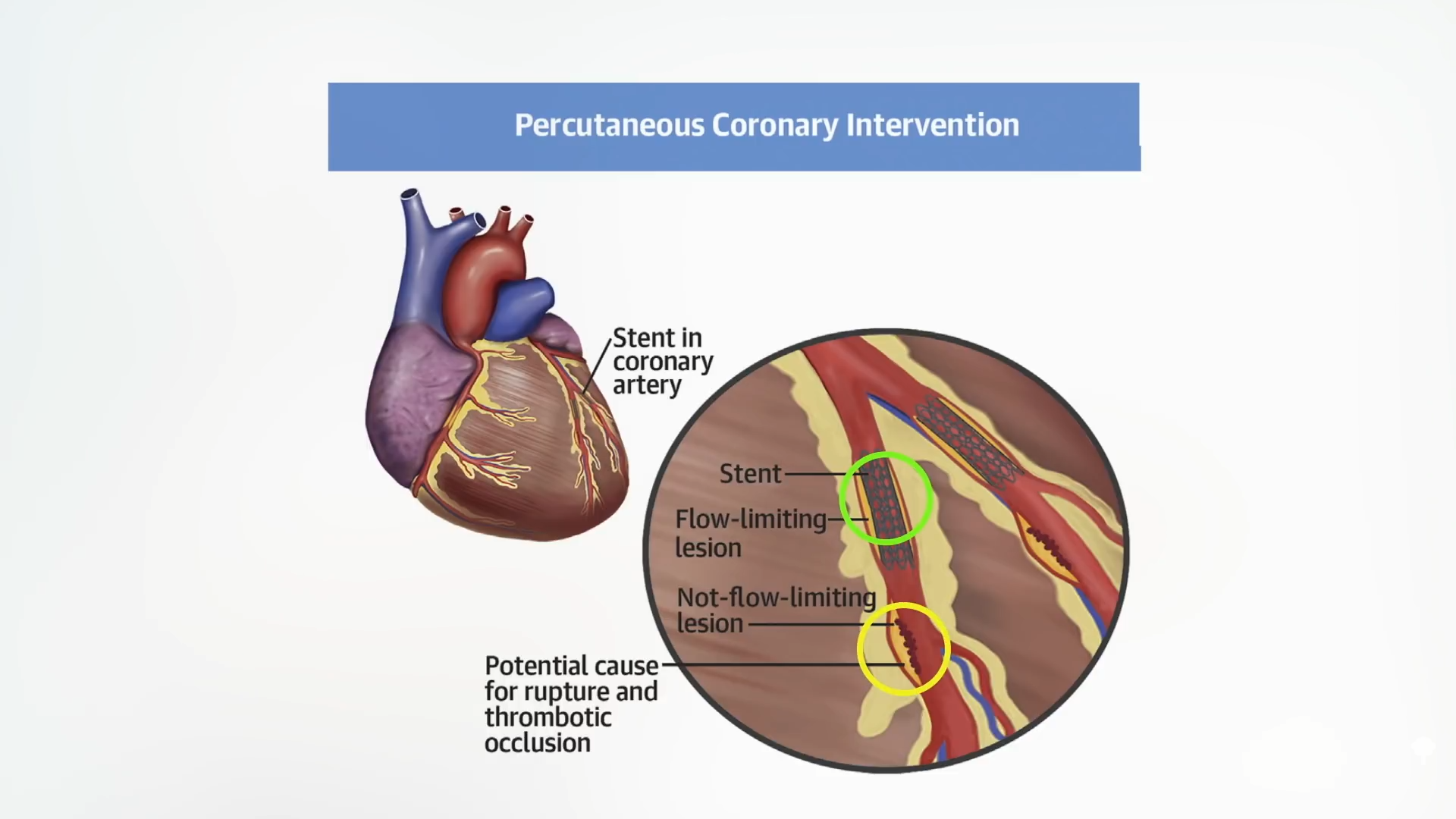
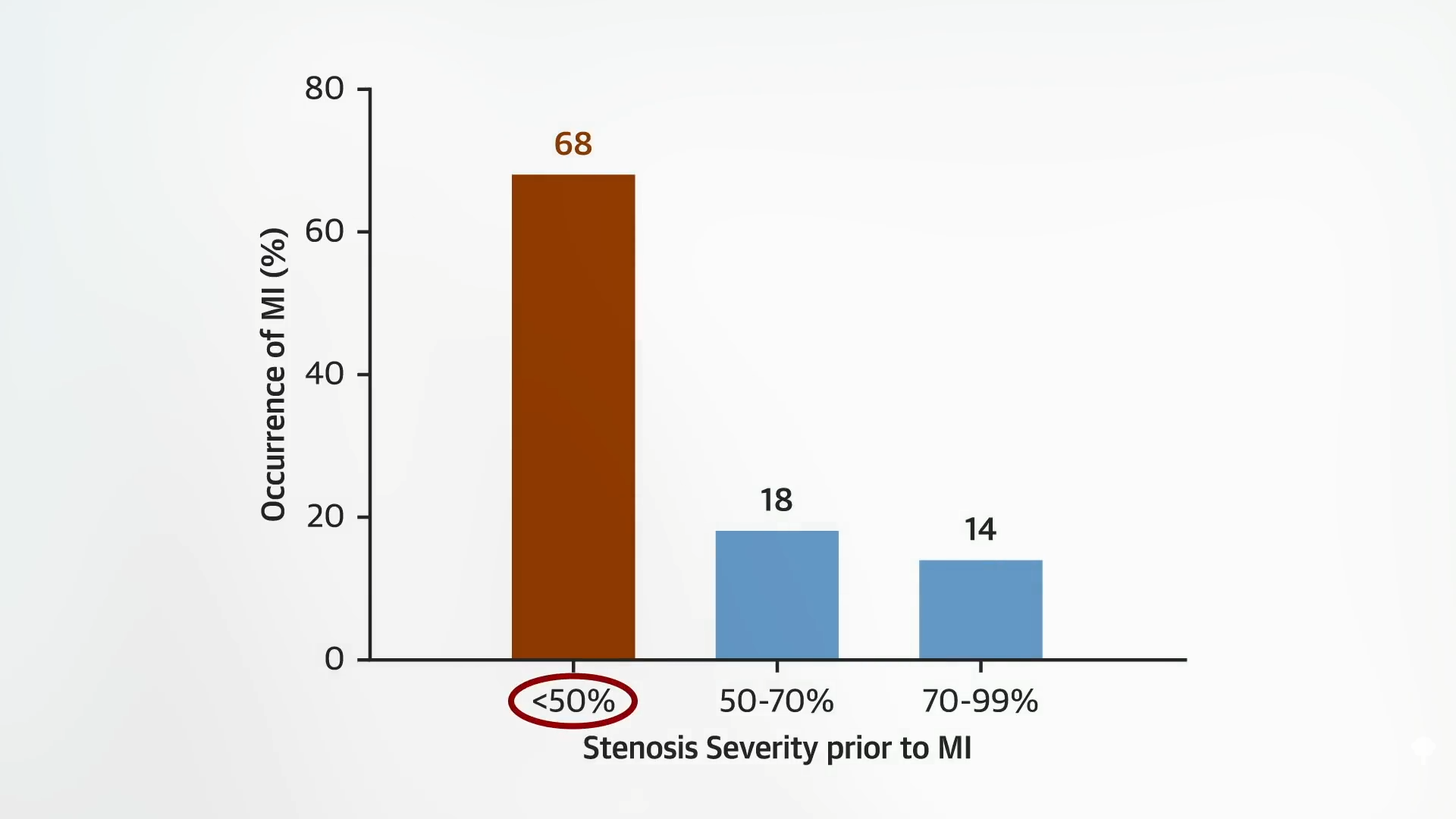
Certainly, most coronary heart assaults are attributable to nonobstructive plaques that don’t even lower blood stream by 50 p.c, as seen under and at 3:40 in my video.
There’s a false impression, a “clogged pipe analogy of secure coronary coronary heart illness [that] has been significantly tough to dislodge,” during which ldl cholesterol plaques slowly and inexorably encroach on blood stream, finally chopping it off utterly and triggering a coronary heart assault. In actuality, “coronary artery illness…is an inflammatory illness during which ldl cholesterol from the blood is deposited in artery partitions, inflicting an inflammatory response, like a pimple. When these pimples pop, they trigger the blood within the arteries to clot on the website…Earlier than rupture, these plaques usually don’t restrict stream and could also be invisible to angiography and stress checks. They’re, due to this fact, not amenable to percutaneous coronary intervention (PCI),” that’s, to angioplasty and stents. Previous plaques are like “scarred previous pimples.”
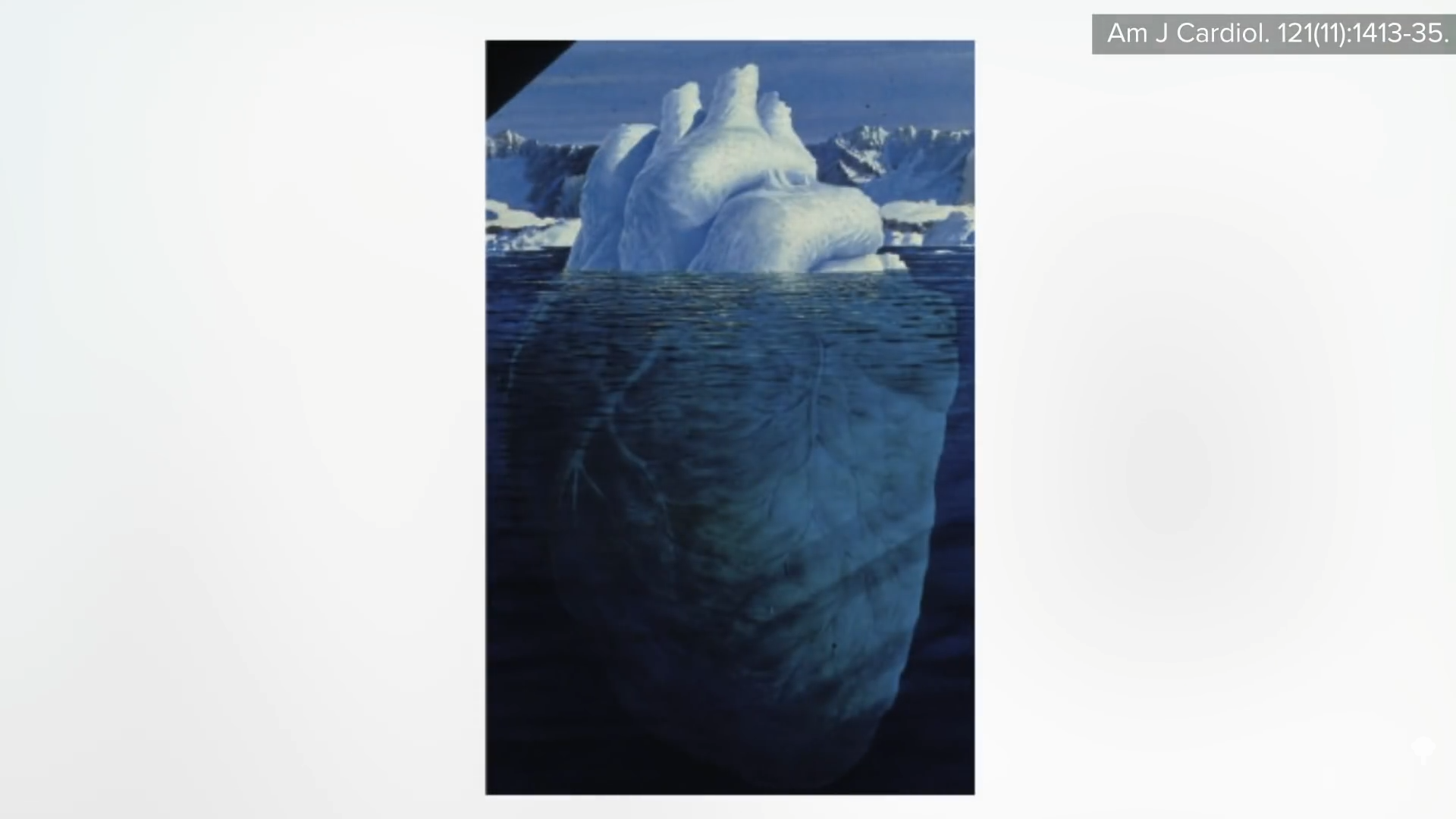
The tightest blockages are made up of largely calcified and dense fibrous scar tissue. They’ll nonetheless rupture and kill us, however there are such a lot of extra of the smaller lesions brewing, that are hidden from view. The way in which we visualize coronary arteries is with an angiogram. X-rays are taken after a black-looking dye is injected into the arteries, so we are able to solely see plaques that encroach on the blood stream. That’s why we get these sorts of tip-of-the-iceberg illustrations, the purpose of which “is to emphasise that a lot of the atherosclerotic plaque within the coronary arteries is just not seen nicely by angiography,” as you possibly can see under and at 4:49 in my video. To essentially perceive what’s happening in folks’s arteries, we should flip to post-mortem. William Clifford Roberts might be essentially the most pre-eminent cardiovascular pathologist on the earth. What did he be taught after finding out coronary arteries for 50 years? After analyzing almost 2,000 our bodies, he discovered that atherosclerosis is a systemic illness.
“In sufferers with deadly coronary artery illness…the amount of plaque is monumental. There isn’t just 1 plaque right here, one other plaque there, with regular lumen [clean arteries] between plaques. Plaques are steady! Not a single 5-mm phase is devoid of plaque” in your entire coronary artery tree. So, says Dr. Roberts: “Remoted coronary illness is a fantasy. There aren’t any things like ‘1-vessel illness,’ and ‘2-vessel illness.’ Plaque is in the entire epicardial coronary arteries whether it is in 1 of them.”
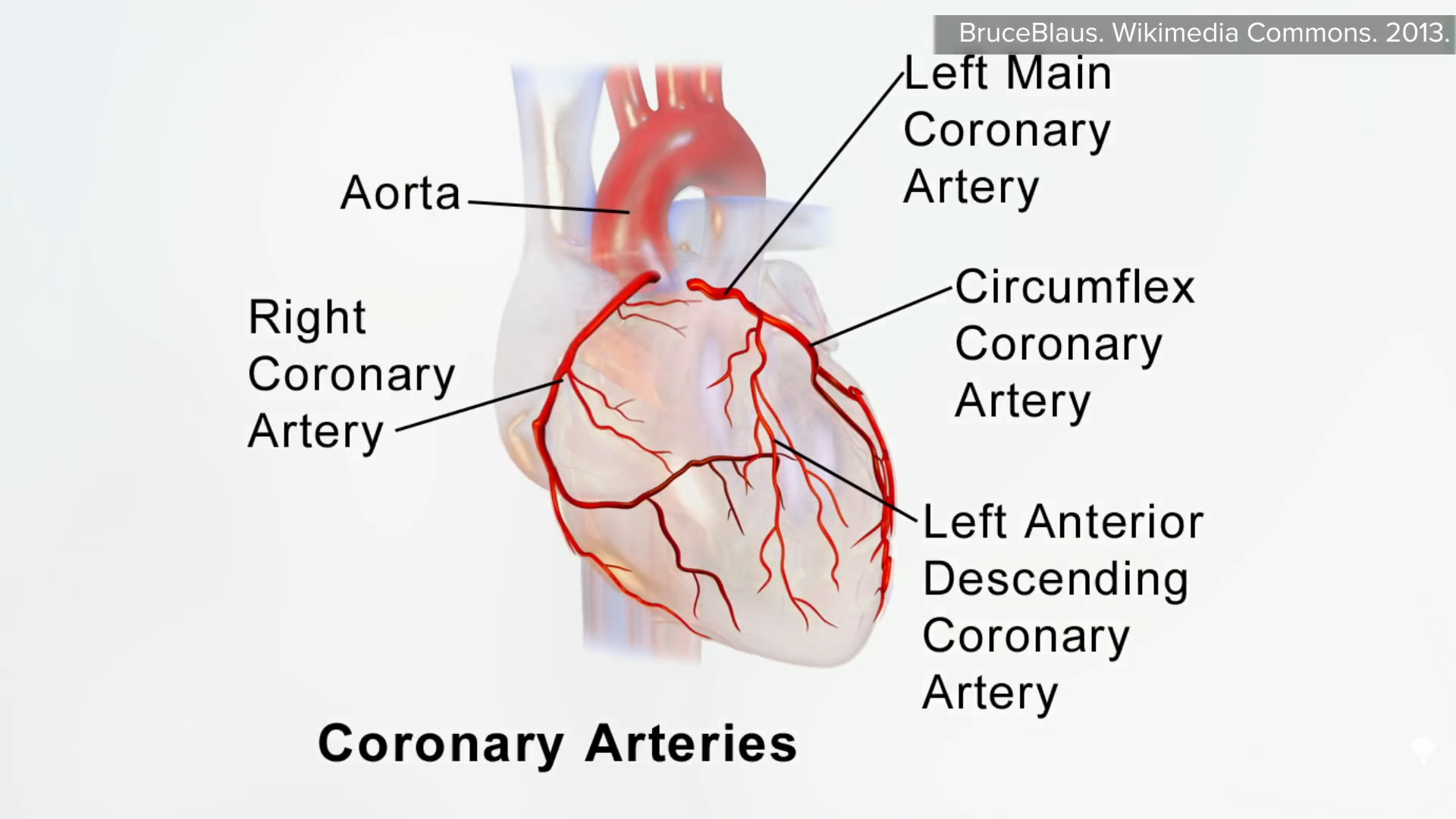
4 predominant coronary arteries feed the guts—the fitting coronary artery, the left predominant coronary artery, the circumflex coronary artery, and the left anterior descending coronary artery, as seen right here and at 6:00 in my video.
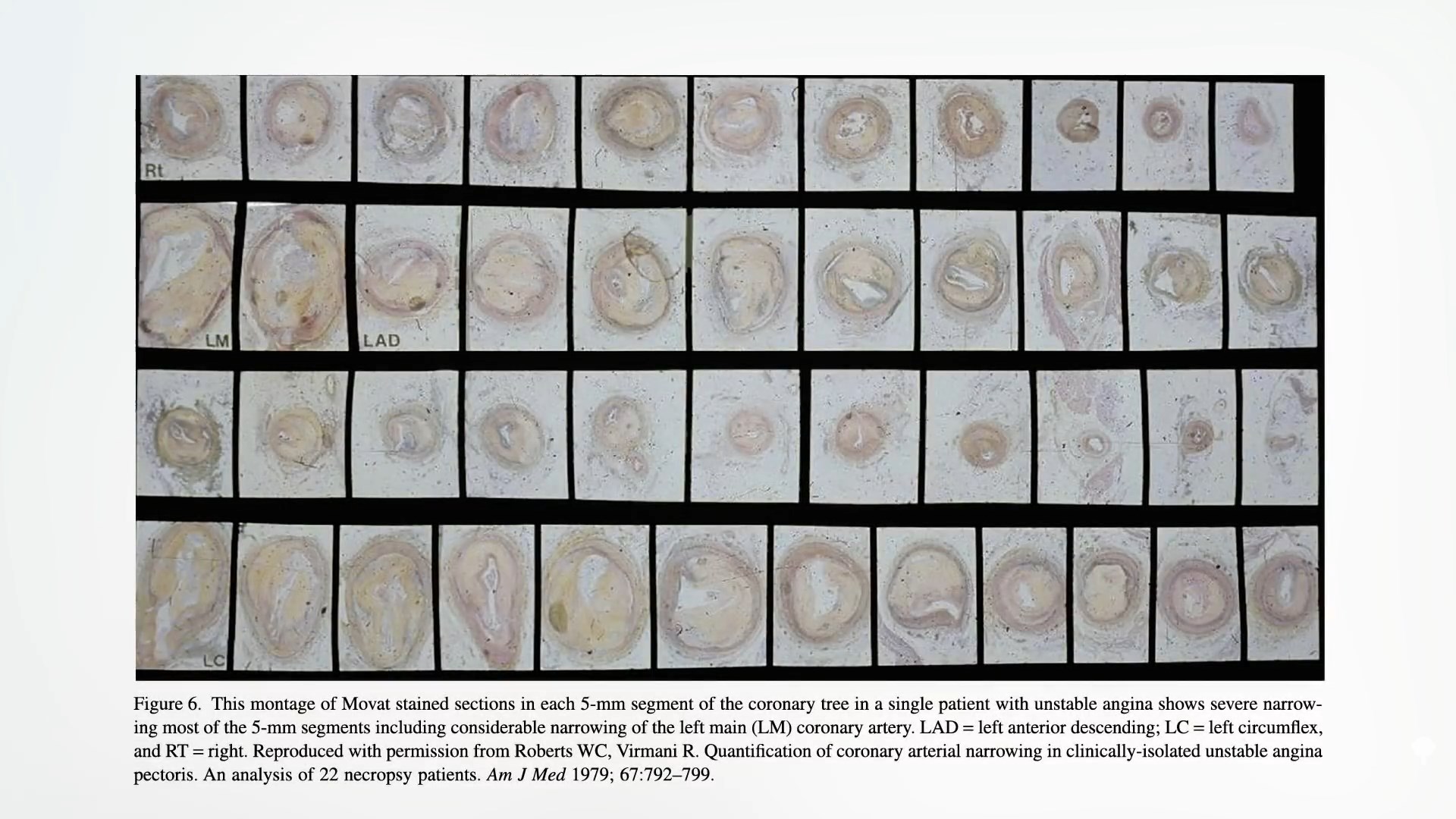
If we add up their lengths, that’s about 11 inches (28 cm) of coronary arteries, which, for examination, might be lower into about 50 quarter-inch (5-mm) slices. Proven under and at 6:17 in my video is what’s seen: Plaque isn’t gunking up one or two slivers however all through all of the coronary arteries. If we have a look at greater than a thousand of those slices from dozens of sufferers who died of coronary heart assaults, “not a single phase was devoid of plaque.” So, it’s no surprise that stenting open in only one space has no affect on coronary heart assaults or demise.






{kind=link}
Discussion about this post